



What is Peroneal Tendon Subluxation/ Rupture?
The Peroneal tendons may dislocate and repetitively subluxation from behind lateral malleolus as a result of trauma in high-end athletes.
- Epidemiology
Mostly peroneal subluxation or dislocation occurs in young, active individuals/ athletes.
- Mechanism of injury
Rapid dorsiflexion of an inverted foot leading to a rapid reflexive contraction of the Peroneus Longus and Peroneus Brevis tendons can tear off the peroneal retinaculum causing subluxation/dislocation of the tendons.
- Pathophysiology
Subluxation of the peroneal tendons leads to longitudinal tears over time which usually involves Peroneus Brevis at the fibular groove. Subfibular impingement is seen occurs secondary to calcaneal malunion at the site of torn superior peroneal retinaculum.
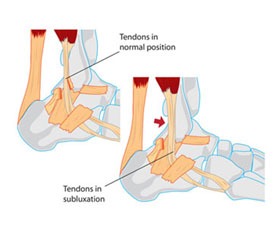
Peroneal Tendon Subluxation
Associated Conditions
This condition may be associated with tears of the Peroneus Brevis and or Peroneus Longus. The tear is mostly longitudinal split than transverse split. In up to 75% of such patients, lateral ankle ligament injuries (Anterior Talofibular Ligament, Calcaneofibular ligament) are also seen with superior peroneal retinaculum tear.
CLASSIFICATION
| Ogden Classification of Superior Peroneal Retinaculum (SPR) Tears | |
|---|---|
| Grade 1 | The SPR is partially elevated off of the fibula allowing for subluxation of both tendons |
| Grade 2 | The SPR is separated from the cartilofibrous ridge of the lateral malleolus, allowing the tendons to sublux between the SPR and the cartilofibrous ridge |
| Grade 3 | There is a cortical avulsion off the SPR off of the fibula, allowing the subluxated tendons to move underneath the cortical fragment |
| Grade 4 | The SPR is torn from the calcaneus, not the fibula |
PRESENTATION
The patient often complains of a popping/ snapping feeling with a dorsiflexion and inversion ankle injury. There is clicking, popping, or snapping and feelings of instability or pain on the lateral aspect of the ankle.
Swelling can be seen posterior to the lateral malleolus. Tenderness can be elicited over the tendons or posterolateral aspect of the ankle on palpation.
A ‘pseudotumor’ like bulging over the peroneal tendons can be seen. Patients can voluntarily subluxation the tendons with or without a popping sound.
Provocative/ Special Test
Apprehension tests
The sensation of apprehension or subluxation with active dorsiflexion and eversion against resistance cause subluxation/dislocation with apprehension.
Compression test
Pain/ apprehension with passive dorsiflexion and eversion of the ankle in patients with superior peroneal retinacular tear.
Imaging
A plain x-ray in an internally rotated view will show a cortical avulsion off the distal tip of the lateral malleolus (fleck sign, rim fracture). The patient should be evaluated for varus hindfoot deformity.
MRI – An axial view of a slightly flexed ankle can demonstrate anatomic anomalies leading to pathologies such as an additional peroneus Quartus muscle or a low-lying peroneus brevis muscle belly.
Treatment of Peroneal Tendon Subluxation / Rupture
- Non-operative:
Short leg cast immobilization and protected weight-bearing for 6 weeks
Indications – all acute injuries in nonprofessional athletes
Technique – tendons of peroneal muscles are reduces reduced at the time of applying the cast.
Outcomes – success rates for nonsurgical management are only marginally better than 50%.
- Operative:
1- Acute repair of superior peroneal retinaculum and deepening of the fibular groove
Indications – acute tendon dislocations in serious athletes who desire a quick return to sports or individuals with an active lifestyle – the presence of a longitudinal tear
2- Groove-deepening with soft tissue transfer and/or osteotomy
Indications – chronic/recurrent dislocation
Technique – if reconstruction of superior peroneal retinaculum tear is not possible, treatment focuses on other aspects of peroneal stability typically involves groove-deepening in addition to soft tissue transfers or bone block techniques (osteotomies to further contain the tendons within the sulcus)
Grafting the Plantaris muscle can be done to reinforce the superior peroneal retinaculum.
The hindfoot varus must be corrected prior to any SPR reconstructive procedure.