



Types of Shoulder Pain
Shoulder Joint and Associated Conditions
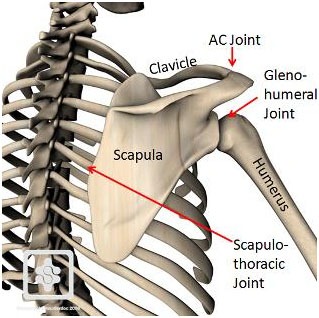
The bony segments of the shoulder complex consist of – The Clavicle, the Scapula, and the Humerus. These segments are joined by three interdependent linkages, namely
- The Sternoclavicular (SC) joint,
- The Acromioclavicular (AC) joint and
- The Glenohumeral (GH) joint.
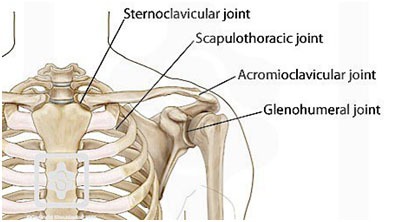
Besides these three joints two functional joints mentioned below are also part of shoulder complex. Though, these are pseudo joints as they don’t have the characteristic of fibrous, cartilaginous or synovial joint.
- The Scapulothoracic joint and
- The Subacromial joint
STERNOCLAVICULAR JOINT:
The Sternoclavicular (SC) joint serves as the only structural attachment of the clavicle, scapula and the upper extremity to the axial skeleton. Movement of any of the bony segment produces movement at this joint. The medial end of clavicle articulates with the notch present on the manubrium sterni at the superolateral (upper outer) end and with first costal cartilage.
The SC joint has a fibrocartilaginous disc that increases the congruency between joint surfaces. The SC joint is surrounded by a fairly strong fibrous capsule. The ligaments that support the joint are-
- The Costoclavicular ligament and
- Anterior and posterior Sternoclavicular ligament.
ACROMIOCLAVICULAR (AC) JOINT:
The lateral end of clavicle articulates with a small facet on the acromion of the scapula to form the AC joint. The angle of contact varies from 16-36 degrees from vertical. Closer the angle to vertical more prone is the joint to wear and tear.
It is a plane synovial joint. The primary function of the joint is to allow the scapula additional range of rotation on thorax.
A joint disc may or may not be present and if present it may vary individual to individual. The capsule is weak and cannot maintain the integrity of the joint without reinforcement of the ligaments. The ligaments are-
- The superior and inferior Acromioclavicular ligament and
- Coracoclavicular ligament
SCAPULOTHORACIC JOINT:
It is formed by the articulation of scapula with the thorax. Anatomically it is not a true joint as it has none of the usual joint characteristic. The articulation of scapula with the thorax depends upon the integrity of the AC and SC joints. Any movement of the scapula will produce movement at these joints. The scapula is maintained on the posterior wall of thorax between 2nd to 7th ribs by the muscle groups attached to it in all directions.
GLENOHUMERAL (GH) JOINT:
The GH joint is a ball and socket synovial joint. This is a highly unstable joint for the sake of greater amount of mobility. As the articular congruency is very less, it’s subsequently susceptible to degenerative changes.
The head of humerus articulates with the glenoid fossa. The glenoid fossa is 1/3rd of the head of humerus, therefore, the acromion, the coracoids and the coracoacromial ligament forms the secondary socket for the head of humerus. Moreover, the laberal attached to the glenoid cavity rim increases the congruency of the joint.
The joint is surrounded by a large capsule that is taut superiorly and slack anteriorly and inferiorly in the resting position of arm. The capsule surface area is twice that of humeral head owing to its greater mobility. The capsule is reinforced by the ligaments, namely-
- The superior, middle and inferior GH ligament
- The Coracohumeral ligament
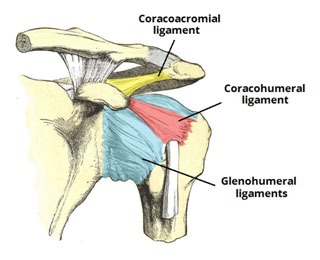
CORACOACROMIAL ARCH:
The coracoacromial (or suprahumeral) arch is formed by the acromion, the coracoids process and the coracoacromial ligament that connects the two bony fragments. It forms the Subacromial joint which provides movement of humeral head underneath the coracoacromial arch. This is again a false (pseudo) joint and named purely on functional basis. This bony-ligamentous vault covers the subacromial bursa, the rotator cuff tendons and long head of biceps underneath it.
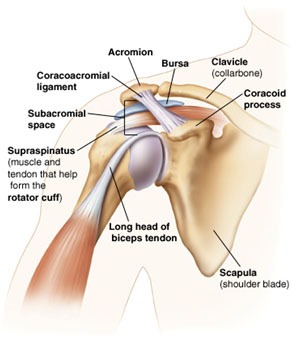
The arch prevents the head of humerus from dislocating superiorly; however, the contact of humeral head with underlying structures can cause painful impingement or mechanical abrasion of the structures lying in the Subacromial space. The Supraspinatus muscle in particular is vulnerable because of its position.
The factors that can cause narrowing of subacromial space and compromise the underlying structure are-
- Anatomical faults like angular variation of acromion inferiorly,
- Change in the slope of acromion,
- Acromion bone spurs,
- AC joint osteophytes,
- A large coracoacromial arch,
- Abnormal scapular or humeral head movement can functionally reduce the size of subacromial space, or
- Inflammation, fibrosis and thickening of soft tissues due to repetitive injury (impingement).
Most Shoulder Pain fall into Four major Categories:
- Bursitis
- Tendonitis/ tendon tear
- Laberal tear
- Instability
- Arthritis and
- Fracture
Other much less common causes of shoulder pain are tumors, infection and nerve-related problems.
BURSITIS
(Subacromial and subdeltoid bursae – The two bursa may be separate but are commonly continuous with each other, hence collectively the two are known as subacromial bursa).
Bursae are small, fluid-filled sacs located around joints throughout the body. They act as cushions between bones and the overlying soft tissues, and help reduce friction between the gliding muscles and the bone.
Excessive use of the shoulder leads to inflammation and swelling of the bursa underlying the subacromial space due to any of the factors mention above. The result is a condition known as subacromial bursitis. Bursitis often occurs in association with rotator cuff tendonitis. Activities of daily living such as combing or getting dressed may become difficult.
TENDONITIS
A tendon is a cord like structure that connects muscle to bone. Mostly tendonitis results from repetitive overuse causing wear and tear over time, much like the wearing process on the sole of a shoe that eventually splits from overuse.
If the tendonitis is not addressed inappropriate time it develops into tendinosis (degenerative changes are seen in the tendon) and is difficult to manage.
The most commonly affected tendons are the 4 rotator cuff tendons and one of the biceps tendons. The rotator cuff is made up of four small muscles and their tendons that cover the head of the humerus and keep it in the shoulder socket. The rotator cuff mainly helps provide stability to the joint.
TENDON TEAR
The tendon may split or tear following a traumatic injury or degenerative changes in the tendons due to advancing age or from long-term overuse and wear and tear. It may be partial tear or complete tear (full thickness tear of the tendon). In complete tear, the tendon is pulled away from its bone attachment. Rotator cuff and biceps tendons are most commonly injured in shoulder joint.
IMPINGEMENT
Shoulder impingement occurs when the head of shoulder impinges the structures underlying the coracoacromial arch when the arm is repetitively lifted overhead. This can lead to bursitis and tendinitis, causing pain and limiting movement. Over time, severe impingement can even lead to a rotator cuff tear.
INSTABILITY
This condition may result from sudden trauma or maybe as a result of hyperlaxity. The head of humerus is either voluntarily (in cases of hyperlaxity) or post injury (due to compromised static and dynamic stabilizers) is forced out of the shoulder socket. The condition may present as subluxation (partial dislocation- which patient can reduce voluntarily) or dislocation (complete head out of socket- needs medical intervention).
If the condition is not addressed with proper rehabilitation, dislocations can occur repeatedly causing recurring dislocations which may be partial or complete. Repeated episodes of subluxation or dislocation increase the risk of arthritis in the joint.
FRACTURES
Shoulder fractures commonly involve the clavicle (collarbone), humerus (upper arm bone), and scapula (shoulder blade). Fractures of scapula or clavicle can be cured with brief period of immobilization as bones are well protected under lots of muscles. Clavicular fractures at times go unnoticed as is associated with minimal pain. A bandage in figure of eight can easily immobilize the clavicle. Clavicular malalignment is the complaint of most patients after fracture reunion. Though it’s a cosmetic issue surgery can be under taken in young females.
Humerus fractures in elderly population are often the result of a fall from standing height while in younger population it results from high impact trauma, such as a motor vehicle accident or contact sports injury.
Fractures often cause Severe Shoulder Pain, Swelling, and Bruising of the shoulder.
We shall not be discussing all fracture around any joint, however, the post immobilization rehabilitation/ or post surgical rehabilitation of fractures will be discussed under separate topic.
The various conditions of Shoulder Pain can be summarized as Under:
Rotator Cuff
- Rotator Cuff Syndrome
- Rotator Cuff Tear
- Bicep Tendonitis
- Shoulder Impingement
- Shoulder Tendonitis
Adhesive Capsulitis
- Shoulder Bursitis
- Shoulder Dislocation (Instability)
- Acromioclavicular (AC) Joint pain
- Osteoarthritis shoulder
Muscle Conditions
- DOMS – Delayed Onset Muscle Soreness
- Muscular Strain
- Overuse Injuries
- RSI – Repetitive Strain Injury
Systemic Conditions
- Fibromyalgia
- Rheumatoid Arthritis
Referred Pain
- Neck Arm Pain
- Pinched Nerve
- Thoracic Outlet Syndrome